From technical validation to its effect on daily reporting
A recently published study in the Journal of Pathology Informatics gives a practical example of what a pathologist needs before accepting any AI tool into routine diagnosis. The issue goes beyond the accuracy of an algorithm shown at a conference or tested on selected images in isolation. The tool was placed inside a fully digital practice for evaluating prostate needle biopsies, then its effect after implementation was measured by report turnaround time and IHC use.
The summary published by Pathology News describes a study from an academic center that had adopted a fully digital practice and performed institutional validation of a decision-support tool for prostate biopsies. The study used pathologists’ diagnoses as the reference standard, then moved the tool into daily work. The researchers then compared prostate biopsy cases during the three months before implementation with the three months after implementation, excluding the transition month so that the adaptation phase would not be mixed into the implementation results.
That design matters. Much of the discussion around AI in pathology stops at sensitivity and specificity. Those figures are necessary, but on their own they do not answer the laboratory’s questions: Will reporting time fall? Will the need for additional stains decrease? Will diagnostic responsibility remain clear? This study tried to measure those questions inside a real workflow.
The numbers that matter to pathologists
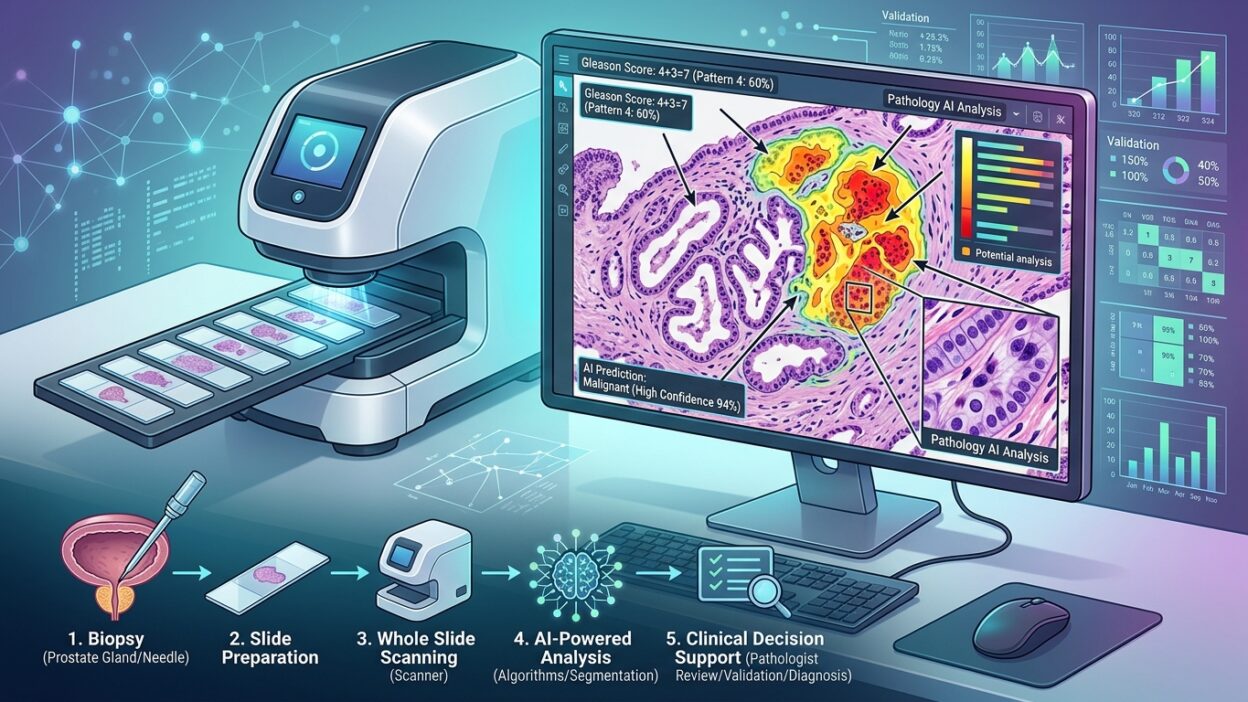
During validation, the tool met the predefined acceptance criteria. Sensitivity ranged from 91% to 100%, specificity was 99%, the positive predictive value was 98%, the negative predictive value was 96%, and the AUC was 0.97. These are strong results, but their practical value is clearer when they are linked to what happened after the tool entered routine sign-out.
After implementation, diagnostic turnaround time fell by 30%, and IHC use fell by 38%. For a department receiving a large volume of prostate biopsies, both figures touch the workload directly. Shorter reporting time means faster movement of cases from scanning to sign-out. Lower IHC use saves cost and removes extra steps, from waiting for sections to the hesitation in cases that a pathologist can resolve on H&E with visual support from the tool.
These results need professional caution. The tool did not become a replacement for the pathologist, and it was not presented as a way to remove diagnostic judgment. The researchers described it as an assistant inside a digital workflow, with the final diagnosis remaining with the pathologist. That point is a condition for trust, not a minor administrative detail. The value here comes from organizing attention and speeding work in an area known for high case volume and repeated need for IHC.
Why prostate biopsies in particular?
Prostate biopsies are well suited for testing this type of tool because they combine high workload, a repeated diagnostic pattern, and frequent need for supporting stains in small or equivocal foci. In a digital environment, the tool can help triage suspicious regions or highlight small foci that require close review. Any claimed benefit, however, must be measured at the case and report level, not at the image level alone.
The reduction in IHC raises an important question: did the tool reduce unnecessary stain orders because it increased the pathologist’s confidence in H&E, or because it helped identify the cases that truly deserved stains? The summary is not enough to answer that in detail, but it gives a signal that every laboratory considering a similar implementation should track. Counting stains alone is not enough. Laboratories also need to monitor concordance, review requests, later report amendments, and disagreement cases discussed in multidisciplinary meetings.
Institutional validation is the starting point
The strongest part of the study is that it does not separate performance from the implementation environment. Institutional validation in digital pathology cannot be reduced to a test on an image set. The laboratory has to test the tool on its own tissue, scanners, section quality, staining patterns, and case distribution seen by its pathologists every day. Prostate biopsies in a busy academic center may differ from prostate biopsies in a small referral laboratory or in a health system that uses a different staining pathway.
For that reason, a high AUC shown by the vendor is not enough. The more important departmental questions are: What defines an acceptable case? What sensitivity threshold is required before use is allowed? Which cases are excluded? How are pathologist comments recorded? Who reviews errors when they appear? These questions sound operational, but they determine whether the tool will help or add another layer of uncertainty.
Implementing the tool after validation and then measuring the before-and-after effect is a good practical step. Even so, each department needs a plan for continuous monitoring after launch. Performance may change with software updates, scanner changes, differences in tissue preparation, or shifts in the case mix over time. AI in diagnosis is not a device that is installed and then forgotten. It needs a clear quality file, like any other part of the laboratory.
A direct effect on department management
From a management perspective, a 30% reduction in TAT may change work allocation, especially if the department has a backlog of biopsies or too few pathologists. The real effect depends on where the bottleneck sits. If the larger delay is in histologic preparation or scanning, a diagnostic tool alone will not be enough. If the bottleneck is waiting for IHC, reducing stain use may matter more than reducing reading time itself.
That is why departments considering similar tools should measure the whole pathway: block processing time, scanning time, WSI availability time, reading time, IHC ordering, return of stained sections, and final sign-out. Only then can the department know whether the tool is solving a real laboratory problem or improving one limited part of the pathway.
What should be followed after this study?
The practical point is not limited to prostate biopsy. This study gives a model for testing any AI tool in pathology: local validation with predefined acceptance criteria, controlled introduction into daily work, and measurement of clinical and operational effects that the department can understand. That is better than relying on external performance curves when the laboratory does not know how they will translate into its day-to-day work.
For the pathologist, the professional question is where AI changes a decision, shortens a step, or reduces an unnecessary stain without weakening diagnostic responsibility. In prostate biopsies, the published numbers are encouraging: high sensitivity, 99% specificity, AUC 0.97, followed by clear reductions in TAT and IHC after implementation. But the final decision for any laboratory should be based on local validation and continuous monitoring, not on the results of one center alone.
Source: Pathology News.