Source: Nature Medicine, April 29, 2026. Original paper: An agentic framework for autonomous scientific discovery in cancer pathology.
I will start with the direct takeaway, because this paper can look complicated if it is read from the AI side rather than from the pathology side.
SPARK is a system that tries to turn a pathologist’s observations on a slide into measurable digital markers. It is not meant to provide a ready diagnosis. It is not meant to replace the pathologist. Its role is to take a digital H&E image, analyze where cells are and how they relate to one another, then propose tissue-based measurements that can be tested against prognosis or a specific biomarker.
The idea in simple terms
A pathologist sees many things on a slide: lymphocyte density, the shape of the tumor border, the relationship between tumor and stroma, inflammatory cells near tumor cells, and variation in nuclear morphology from one area to another. We use many of these observations mentally while reading a slide, but we do not always measure them as precise numbers across thousands of cases.
SPARK tries to do that digitally.
Instead of asking an AI model one question, such as whether a tumor is MSI-high, SPARK tries to ask many histologic questions, such as:
- Are lymphocytes close to tumor cells or far from them?
- Do tumor cells at the tumor edge differ morphologically from tumor cells in the center?
- Is there a specific pattern in the distribution of macrophages or fibroblasts around the tumor?
- Is the tumor-stroma relationship associated with lymph node metastasis or survival?
It then turns each of these questions into a number. That number becomes a parameter that can be tested statistically.
What goes into SPARK?
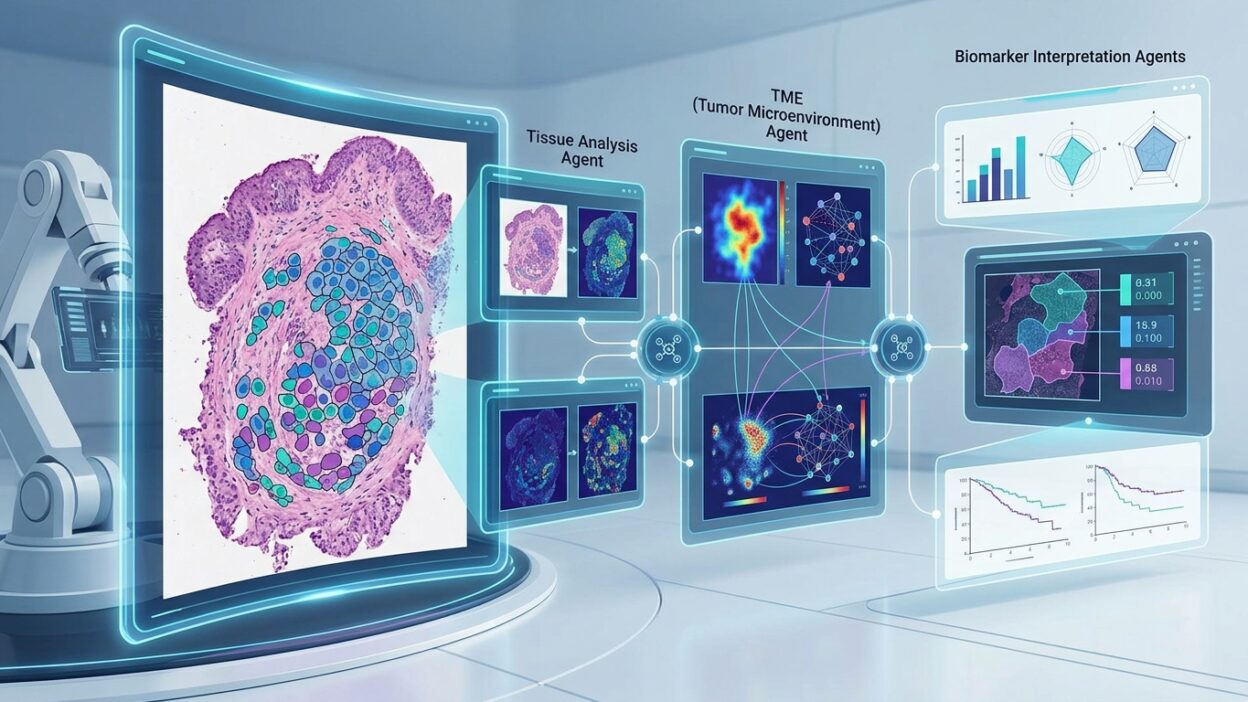
SPARK takes whole-slide images from H&E sections after digital preprocessing. Before SPARK starts, the image has already gone through familiar image-analysis steps: identifying tumor regions, separating tumor from stroma, and recognizing main cell types such as tumor cells, lymphocytes, macrophages, neutrophils, fibroblasts, and others.
In other words, SPARK does not start from a raw image alone. It works on top of a digital map of the slide: where the tumor is, where the stroma is, where the cells are, and an approximate type for each cell.
What does it produce?
The main output is not a diagnosis. It is a long list of digital markers. Each marker represents a specific histologic idea.
A simple example: if the idea is “lymphocyte proximity to tumor cells,” SPARK turns it into a measurement, such as the mean distance between lymphocytes and tumor cells, the number of lymphocytes within a defined distance from tumor, or the difference in this pattern between the tumor center and invasive edge.
The researchers can then test whether this number is associated with prognosis, PD-L1, MSI prediction, or separation between high-risk and low-risk patients.
Where does agentic AI fit in?
The word agentic here means the system is not a single step. More than one agent works in sequence. One agent proposes the biological idea, another refines it, another converts it into code, and then a validation step checks that the resulting marker is computable and is not redundant or unhelpful.
Think of it as a small team working with the pathologist:
- The first suggests histologic questions.
- The second turns the question into a more exact definition.
- The third writes the measurement method.
- The fourth tests whether the measurement actually works on the data.
This is the difference between SPARK and a traditional classification model. A traditional model gives you an output. SPARK tries to create new markers that can be understood and discussed.
What did the researchers find?
The researchers tested the system on more than 5,400 patients from 18 cohorts and five cancer types: lung adenocarcinoma (LUAD), lung squamous cell carcinoma (LUSC), colon adenocarcinoma (COAD), breast cancer (BRCA), and head and neck squamous cell carcinoma (HNSC).
SPARK generated hundreds of histologic ideas. After the ideas were converted into code and redundant or impractical markers were removed, the team had more than a thousand digital markers that could be tested.
Some of these markers were associated with features that pathologists and oncologists know well, including grade, ER status in breast cancer, HPV/p16 in head and neck cancer, MSI in colon cancer, and PD-L1 in lung adenocarcinoma.
Why does this matter?
The point is not that SPARK outperformed every model or is ready for clinical use. The point is that it gives a different way to think about AI pathology.
Many AI models in pathology work as black boxes: an image goes in and a result comes out. The result may be good, but it can be difficult to understand exactly why the model made that decision.
SPARK tries to bring the question closer to how a pathologist thinks. Instead of “the model says the patient is high-risk,” we get something like a specific pattern of lymphocytes and macrophages at the tumor edge, a change in tumor-cell nuclear morphology near the stroma, or a particular distribution of fibroblasts inside the tumor, with those markers linked to prognosis.
That makes the discussion easier: does this pattern make biological sense? Do we actually see it on the slide? Can it be connected to tumor immunity, invasion, or stromal reaction?
A practical example
Suppose we have lung adenocarcinoma and want to understand why some patients have worse outcomes than others. A traditional model may provide only a risk score. SPARK tries to extract several markers, such as the relationship between tumor cells and stroma, the distribution of immune cells, or nuclear morphology at the invasion front.
If high-risk patients repeatedly show a particular pattern, we have a biological lead. The pattern may reflect immune evasion. It may reflect stromal activation. It may not prove the mechanism, but it gives us a hypothesis that can be studied.
Does SPARK diagnose patients now?
No. This is a very important point.
The study is retrospective. Most cases were resections, not small biopsies. The results need prospective validation before any clinical use. Also, some cell classifications on H&E are approximate, especially when we talk about fibroblasts or stromal cells, because H&E alone does not provide precise cell identity in the way multiplex imaging or spatial proteomics can.
For that reason, SPARK should be read as a research and biomarker-discovery tool, not as a ready clinical test.
Where can pathologists benefit?
The main potential benefit is turning pathology ideas into measurements. If you notice a pattern on a slide and want to test it across hundreds or thousands of cases, a system like SPARK can help formulate the idea, write the measurement method, and test its association with clinical outcomes.
This opens an important route in digital pathology: we do not use AI only to classify images. We can also use it to discover new histologic markers that remain interpretable.
Bottom line
SPARK is a digital pathology research framework that tries to do three things:
- Read the cellular and spatial map inside the slide.
- Propose histologic markers based on biological ideas.
- Test whether those markers are associated with prognosis or known biomarkers.
Its value is that it brings AI closer to the pathologist’s way of thinking. Instead of a vague score, we get questions and markers that can be read, reviewed, and connected to tumor biology.
It is not a ready diagnostic tool. But it is a clear example of where the field is heading: AI does not only answer a question. It can help the pathologist generate histologic hypotheses and test them digitally.
In one sentence: SPARK turns slide observations into testable numbers, which may help us discover new morphologic biomarkers from H&E and spatial biology data.