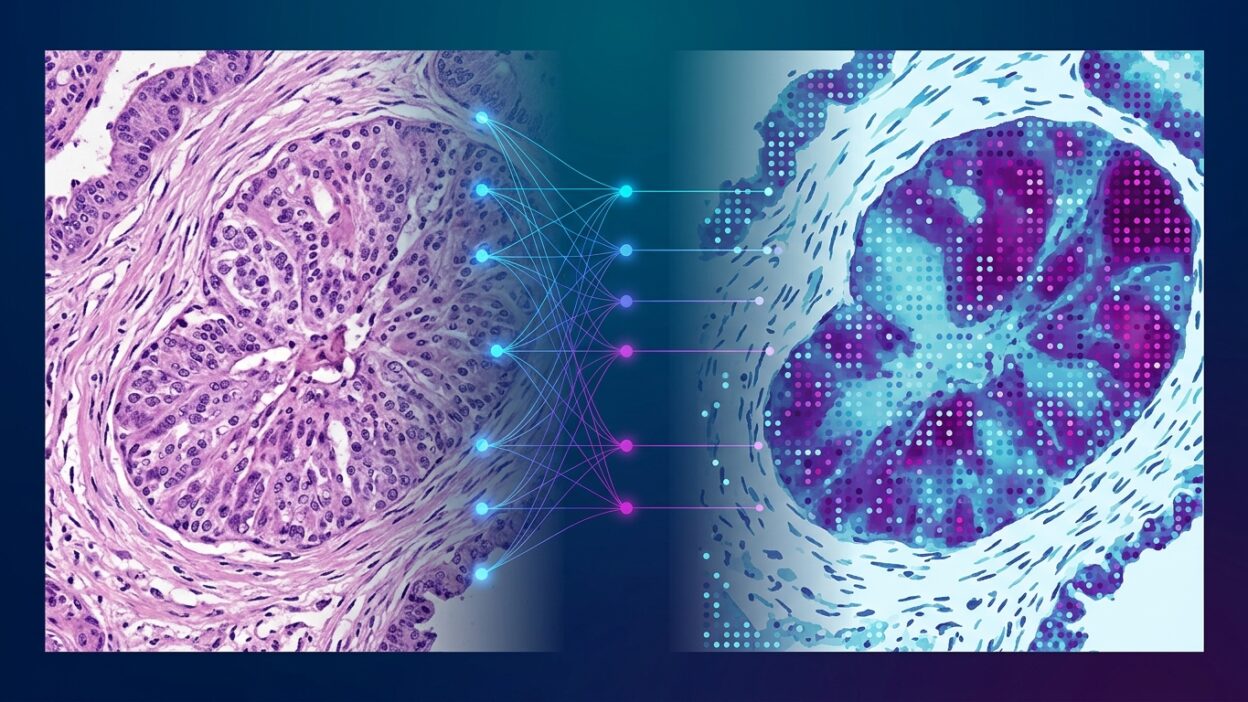
Cell published a study titled AI-predicted spatial transcriptomics unlocks breast cancer biomarkers from pathology. The paper proposes a practical route for expanding the use of spatial data in breast cancer without running spatial transcriptomics on every sample. The direct idea is a deep learning model called Path2Space: it learns from histopathology slides paired with ST data, then predicts spatial gene expression directly from the image.
This kind of work matters for digital pathology because it does not treat the slide only as a classification image. The aim is not to predict tumor grade or a ready-made subtype. It is to build a predicted spatial molecular layer on top of the tissue, so tumor architecture and the TME can be analyzed across large cohorts that cannot realistically all be tested with costly ST methods.
The difference from many earlier WSI models is that the output is not a single slide-level or tile-level label. The output is an expression map. The question shifts from “what is in the sample?” to “where does the molecular signal appear inside the sample?” That shift brings the model closer to the language of pathology, because slide interpretation always starts with location and the relationships between components.
What did the researchers do?
Shulman and colleagues introduced Path2Space to predict the spatial expression of thousands of genes from breast cancer slides. According to the study abstract, the model was trained on a broad set of breast cancer spatial transcriptomics data, then compared with 21 published methods. It performed better in the task of predicting spatial gene expression, then was used to map the tumor microenvironment in 976 tumors from TCGA.
The important step is not only the numerical comparison. Applying the model to TCGA turns an archive rich in clinical follow-up and molecular data into a space where spatial hypotheses can be tested at a scale that was not previously available. Usually we have H&E and bulk omics data, but we lack the spatial organization of gene transcription inside and around the tumor. Path2Space tries to fill that gap with an image-derived prediction.
From image to measurable TME map
The study states that the model accurately inferred the abundance of cell types within the TME and identified three spatial clusters in breast cancer that were associated with survival differences. This point is sensitive for pathologists: the stratification is not based on morphology separated from biology, and it is not based on bulk RNA that erases location. It tries to connect tissue pattern, gene expression, and the spatial distribution of cells.
If these findings hold in external cohorts and across different imaging protocols, we may have a new framework for extracting biomarkers from archived slides. Not a direct replacement for HER2 IHC, ISH, or validated gene-expression tests, but an added layer that may reveal spatial relationships that do not appear in sample-level averages.
Treatment response: where does the map help?
One of the paper’s strongest claims is that low-cost spatial maps extracted from H&E through Path2Space improved prediction of response to chemotherapy and trastuzumab compared with conventional markers based on bulk sequencing. That claim needs critical reading when the full text and detailed data are available, but it puts an important question in front of the field: is location itself a biomarker?
In breast cancer, the position of immune cells, areas of hypoxia, contact between tumor cells and stroma, and heterogeneity of expression within the mass may matter more than the overall average of some genes. Pathologists see these relationships every day, but turning them into quantitative variables linked to treatment response has been difficult. Models such as Path2Space try to translate that visual judgment into spatial gene maps that can be tested.
What should we not conclude too quickly?
The study does not mean that ST is no longer needed. The model learns from ST and is affected by training quality, platform type, tissue preparation, scanner, staining, and case distribution. Predicting gene expression from an image also remains a probabilistic prediction, not a direct measurement. Any clinical use will need independent validation, clear performance standards, and analysis of model failure in rare cases, treated tumors, or slides with extensive necrosis.
There is also the question of portability. A model trained on breast cancer may not carry the same quality to other tumors without suitable training data. Even within breast cancer, differences in subtypes, prior treatments, and slide quality may change the signal. For now, the nearest value appears to be in translational research and hypothesis generation across large archives, rather than as a ready clinical decision tool.
Why this matters for digital pathology
The practical value of Path2Space is that it redefines what can be extracted from H&E. The slide is not merely an input for a classification model. It may become an input for building an approximate spatial omics layer over thousands of archived cases. That opens the door to biomarker discovery experiments at a scale that would be too expensive if they relied entirely on ST.
For pathologists, the direction is clear: upcoming models will not stop at saying “cancer” or “not cancer.” They will move toward describing tumor biology spatially, linking tissue structure with gene transcription, treatment response, and clinical outcomes. The professional question will not be whether the algorithm replaces slide reading. It will be how we review its maps, test its limits, and decide when it adds information beyond morphology, IHC, and molecular testing.
Bottom line
Path2Space is a mature example of an important direction in digital pathology: turning routine slides into predicted spatial molecular maps. The paper does not close the file on spatial transcriptomics. It suggests a way to use ST as training data, then extend some of its signals to large H&E cohorts. If the results hold in external validation, this approach may become a strong tool for discovering treatment biomarkers in breast cancer, and later perhaps in other tumors.
Source: Shulman ED et al. Cell. 2026. DOI: 10.1016/j.cell.2026.04.023.